THIS IS SHIVANI NAYINI OF 2018 BATCH CURRENTLY DOING POSTING IN GENERAL MEDICAL DEPARTMENT
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of “ patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Cases I have documented
CASE 1
blog-
https://shivaninayini104.blogspot.com/2023/10/this-is-online-e-log-book-to-discuss_14.html
Chief Complaints:
Bilateral loin pain since 3days.
History Of Presenting Illness:
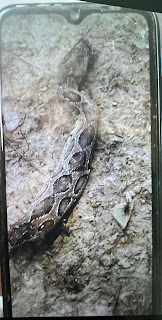
Patient was apparently asymptomatic 7days back then he sustained snake bite (with Russell viper) on left ring finger while working in the fields,visited local hospital and managed symptomatically.
C/O bilateral loin pain,insidious in onset ,intermittent,gradually progressive,pricking type ,non radiating,aggravates on lying down.
C/O low grade fever,Nausea and vomiting,bloating.
N/C/O Burning Micturation,decreased or increased urine output.
N/C/O cough,cold,body aches,chest pain.
(17-10-23) SOAP NOTES
Ward patient
S : B/L loin pain since 10days
Decrease in right sided loin pain.
O :
Patient is conscious coherent cooperative
Vitals :
Temp. : 98.2F
PR : 90 bpm
RR : 17 cpm
BP : 130/100 mm Hg
SpO2 : 98% @ RA
CVS:S1S2 heard
R/S: BAE +
P/A:soft,tenderness in left lumbar region.
CNS:NFND
A :Non oliguric Acute Kidney Injury (resolved) secondary to snake bite.
P : INJ OPTINEURON 1amp in 500ml. NS/IV/OD
INJ TRAMADOL 1amp in 100ml NS iv /BD
PaJR-
https://chat.whatsapp.com/DqSllI6qLfoH46TGL8spqg
OSCE:
1)List all the complaints of the patient with respect to the history?
Ans-Bilateral loin pain
-nausea
-vomiting
-low grade fever
2)What type of Russell viper venom?
Ans-Hemotoxic
Nephrotixic
3)How Russell viper venom affects the coagulation pathway?
Ans:RVV-V is a glycoprotein with a single N-linked oligosaccharide chain attached at Asn229. Three isoforms of RVV-V have been identified and the two predominant species have been sequenced . The two sequenced isoforms, RVV-Vα and RVV-Vγ, share an overall sequence identity of 98%, differing at just six amino acids, and each of the replacements can be accounted for by a single point mutation in the nucleotide sequence . RVV-V contains 12 cysteines, and six disulfide bonds are postulated on the basis of the homology with other members of the chymotrypsin family. Of the six disulfide bonds one, Cys76-Cys234, is unique to snake venom serineproteinases, being found also in the snake venom proteins batroxobin and flavoxobin , but not in thrombin or any other normal physiologic proteinase. A major difference between RVV-V and other trypsin-like serine proteinases occurs in the highly conserved region close to the catalytic site that contains Ser214 of chymotrypsin . The sequence Ser214-Trp215-Gly216 (chymotrypsinogen numbering) is replaced by Ala197-Gly198-Gly199 (RVV-V numbering). Few other members of the chymotrypsin family (S1) have been found to lack the Ser214-Trp215-Gly216 sequence. The tertiary structure of the complex between RVV-V and a fourteen-residue peptide (residues 1533–1546) from human factor V has been solved. The structure shows that RVV-V interacts with seven residues of the peptide fragment from Arg1545 in P1 to Ile1539 in P7. From comparisons with the structure of the uncomplexed peptidase, conformational changes in some loops are observed upon substrate binding, and an induced fit mechanism has been suggested to explain the narrow specificity of RVV-V .

4)How will you identify poisonous and non posionous snake .

CASE 2
Blog
https://shivaninayini104.blogspot.com/2023/10/this-is-online-e-log-book-to-discuss_28.html
Chief Complaints:
Patient came to casualty with H/O 2-3 episodes of involuntary movements of right upper and lower limb and face since evening(28/10/23)
History Of Presenting Illness:
Patinet was apparently asymptomatic till today afternoon after she which she started having involuntary movements of right right upper and lower limbs associated with up rolling of eye balls and frothing not associated with involuntary micturation and defecation associated with postictal confusion for 15-20min.
H/o seizure activity on and off from past 3years and is on medication.
No h/0 fever and head trauma.
K/c/o Hypertension,CVA
SOAP Notes :
Icu bed 1
30/10/23
S : 4 episodes of seizures
Stools passed
O :
Patient is not conscious
Gcs:E1V1M1
Vitals :
Temp : 98.4 F
BP : 120/70 mmHg
PR : 102bpm
I/O : 1570/900 ml
Grbs:175 mg/dl (8U HAI)

A:
Focal seizures with impaired awareness with cva
K/c/o HTN
P :
1.IV FLUIDS NS RL@75ML/HR
2.INJ LEVIPIL 1gm iv/bd
3.INJ SODIUM VALPROATE 500mg iv/bd
4.INJ PRACETAMOL 1gm iv/sos if temp >101F
5.INJ LOREZEPAM 2CC iv/sos
6.INJ PAN 40mg iv/od
7.TAB PCM 650 mg Rt/od
8.NEB MUCOMIST 6th hourly
9. ORAL SUCTIONING 4th hourly.
PaJR-
https://chat.whatsapp.com/KINtknxfGus0T5ZH7pNQw3
CASE 3
https://shivaninayini104.blogspot.com/2023/10/this-is-online-e-log-book-to-discuss.html
Chief Complaints:
Pain abdomen since 2months
History Of Presenting Illness:
Patient was apparently asymptomatic 2months back then she developed pain in hypogastric region which was inscidious in onset,continuous,pricking type,non radiating,no aggravating factors and relieved temporarily on taking pain killers.
C/o bilateral foot and hand tingling sensation since 1year.
C/o burning micturation
No c/o cough,sob,palpitations,
sweating
No c/o vomiting,nausea,loose stools
No c/o polyuria,polydipsia,polyphasic,fatigue
k/c/o DM since 15days
Daily routine:
Wakes up at 6am,does her house work and takes bath and takes breakfast by 8am and takes insulin injection at 10:50am and then takes her her lunch around 11am and then sleeps or watch tv and have tea and biscuits in the evening and then takes insulin injection at 8pm and then takes dinner, does some household work and sleeps by 10pm.
PaJR-
https://chat.whatsapp.com/FXC5MQxFkTa6Ln7oWdfd3
CASE 4
https://shivaninayini104.blogspot.com/2023/10/this-is-online-e-log-book-to-discuss_11.html
Chief complaints:
A 80 year male came to the opd with complaints of pain in hypogastric region since 1year.
Dribbling of urine since 9months
History of presenting illness:
Patinet was apparently asymptomatic 1year back the he developed pain in hypogastric region which is continuous,pricking type ,non radiating no aggravating and relieving factors.
C/O dribbling of urine associated with burning micturation.
C/O urinary incontinence
No C/O vomiting,nausea,fever,cold,cough.
PaJR
https://chat.whatsapp.com/KO0yxST1q4d71H7xkzjUQw
CASE 5
https://shivaninayini104.blogspot.com/2023/10/this-is-online-e-log-book-to-discuss.html

Comments
Post a Comment