14yrs boy with massive splenomegaly
THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE - IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS / HER /GUARDIAN'S SIGNED INFORMED CONSENT .HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS WITH AN AIM TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUT.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
14 year old male came to OPD with chief complaints of
Weakness since 10 days
Fever since 2 days
History of present illness
7 March 2009
1 year old male child was brought with complaints of Not gaining weight since last 3 months
Delayed mile stones since last 3 months, loose motions/ vomitings on & off since 3 months
HOPI : Child was appasently asymptomatic 3 months back than child was not gaining weight, loose motions greenish in colour, watery in character 25- 30 times a day, not associated with blood & mucus, vomitings 4-5 times, non bilious/ non projectile, No history of ear discharge, History of recurrent cough, No history of decrease in urine out put, No history of cyanosis,.
Antenatal history: Mother had regular AN checkups, had 2 doses of T.T, Had IFA prophylaxis, No history of DM/HTN/TB, No history of prom/APH, Birth history: SPVD cryed immeditaly after birth, birth weight 4.25Kgs.
Post nenotal history: MSL NICU admission for 1 day, excsive Breast feeds from 2nd day of life, exclusive breast feeds till 6 months, F/B weahing started with cerelac continued till 10 months, than child had loose motions/, stopped cerelac / Breast feeding started with MCT 130ml for 1 scoop continue only simyl/MC /now also. Now child is not taking glind diet also. Development history: Development was asymptomtic till 10th month than delay in mile stones, Global delay in all fealds with bones. O/E: Child dull, Pulse well felt, HR 90/min, RR 26/min, Heart s1 s2+, Lungs BAe+ clear, P/A soft, old man look, folds skin, loss of buccal pad of fat,
At 9 years of age - parents noticed neck swelling and they took him to ENT doctor later referred to
endocrinologist where he was diagnosed with hypothyroidism - intial TSH was -150, he was started with 150 mcg of thyronorm, later increased to 180 mcg patient also gives history of chronic itching over hands and foot since the age of 9 years.
At 12 years of age patient had chicken pox resolved over 10 days.
At the age of 13 years (06.01.2022)- he came with history of yellowish discoloration of eyes since 9 days. One episode of bilious vomiting. He also complaints of fever ,pain abdomen, loose stools.No cold, cough No history of small joint pains. colored urine .No pale colored stools .No He was treated by a pediatrician for jaundice, but as the bilirubin is increasing they referred here for further management. On examination - He is thin built.Height -156 cm Weight - 32kgs Jaundice + pallor + Per abdomen - moderate splenomegaly was noted
At 14 years of age
He presents to us with the complaints of weakness since 10 days , when the mother noticed child appears to be dull
5 days ago the parents noticed a swelling in the groin and 2 days onwards the child has fever that was insidious in onset, spikes were noted in the morning and night hours associated with body pains. No h/o vomitings , headache or any drug intake.
Child also have
Family history
He is a 4th order child, born out of grade 4 consanguinous marriage He has 2 elder brothers and one elder sister - who expired at 5 years of age His sister was the first child and she was asymoptomatic till 2 years of age,then she had shortness of breath and was rushed to hospital, where the condition detiorated and she got admitted. They were told that she had splenomegaly and her blood counts were decreasing. She was given multiple blood transfusions every 25 days for one year inspite of that she remained anemic,she also underwent bone marrow biopsy twice .According to parents she was given steriods also for one year before death she never had jaundice or recurrent infections.
Elder brother is 19 year old and second brother is -16 years old .Second one had history of fever ,white coloured loose stools at the age of 5 years for which they went to nalgonda hospital.He was given some medications and it got resolved .But he was said to have anemia,and he recovered according to parents with some medications. There was no jaundice and no history of blood transfusion.
General physical examination
Patient is conscious ,coherent and cooperative and well oriented to time, place and person.
moderately built and nourished.
Pallor-present
Icterus-absent
Cyanosis-absent
Clubbing-absent
Lymphadenopathy-present(inguinal,cervical)
Edema-absent
Vitals:
Temperature - 99.5*c
PR :- 89bpm
RR :-20cpm
BP :- 110/80mm Hg
GRBS :-83mg/dl
26/8/22






Systemic examination:
CVS-S1S2 heard no murmurs
RS-BAE+
CNS-NFND
P/A-hard on left side,tenderness present in left hypochondriac,left lumbar and umbilical region.
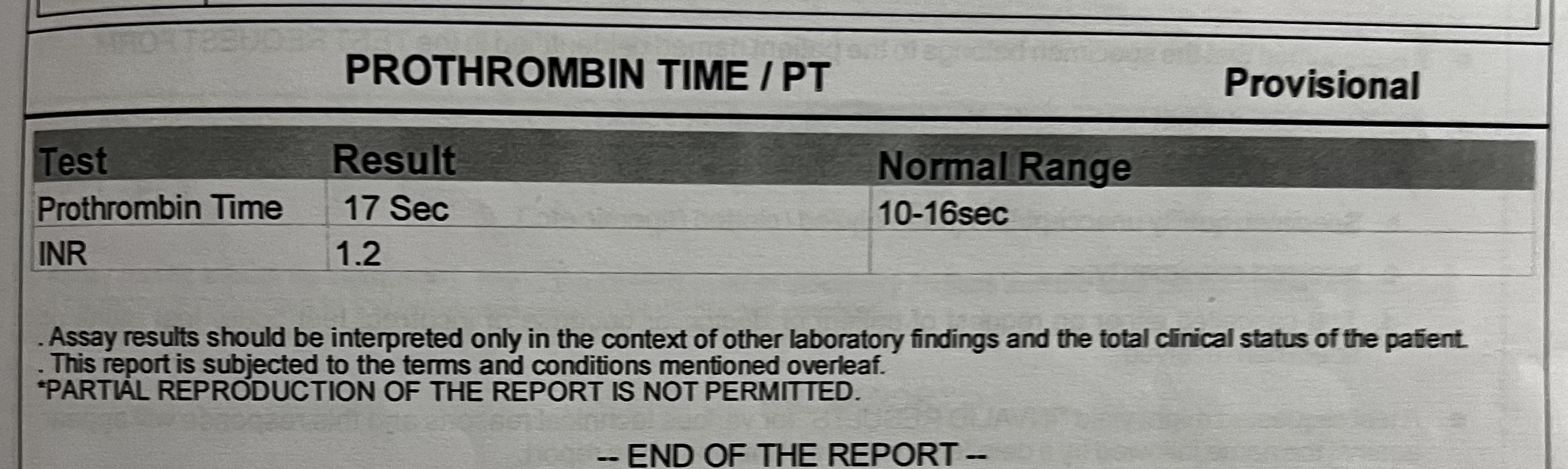
Investigations:











Provisional diagnosis :
Autoimmune hemolytic anemia with thyroidits.
Pancytopenia with massive splenomegaly.
Treatment:
Inj.NEOMOL 1gm iv sos(if temp > 101*F)
Tab Dolo 650 mg po TID
Tab levocitrizine 5mg po sos
Syp Ascorii-D 10ml po bd
Tab thyronorm 20mcg po OD
Inj optineuron 1amp in 100ml NS iv OD

Comments
Post a Comment